Distress
“Distress” refers to the way we respond to situations in the past, present, or future which make us sad, angry, or anxious. How we cope with distress is different for everyone and impacted by our life experiences. Learning of a terminal diagnosis can be a highly distressing experience. People with Learning Disabilities (PWLDs) are more likely to have experienced traumatic life events, experience life events as stressful and have difficulties in processing traumatic events. This means that they are likely already coping with more stress than a person without a learning disability and so may be more likely to show highly increased distress more often than a person without a learning disability. As well as this, previous difficult experiences of death or serious illness impact the distress that people feel when thinking about their own death.
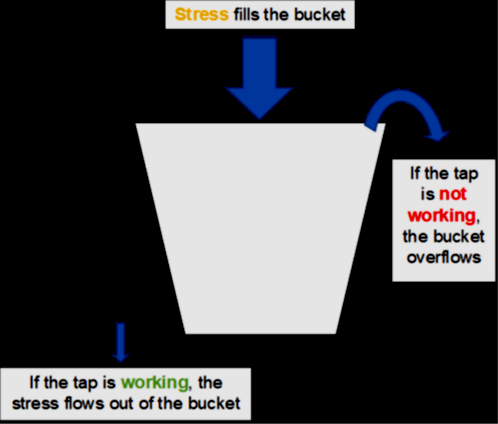
We can think about this using the stress bucket metaphor. We all have different size “buckets” or different amounts of stress that we can handle. When we are too stressed, our buckets overflow and we become distressed. When we do things that make us feel better or use the “tap” our distress becomes more manageable.
Distress & Discomfort Tool (DISDAT)
When someone is distressed or in pain the way they communicate this can be very similar. If the person is in an unfamiliar surrounding like hospital, and anxious then it may be hard to tell if they are distressed because of their surroundings or in pain. This tool allows you to identify someone’s baseline of distress and then compare in other situations to use strategies to reduce their distress.
St Oswald’s Hospice | Distress and Discomfort Assessment Tool (DisDAT) (stoswaldsuk.org)
What distress looks like – People who are distressed may present in two ways:
- They may be visibly anxious (for example – panicky, shaking, breathing very fast), sad (for example -, tearful, upset) or angry (for example – shouting, becoming aggressive). This is known as Hyperarousal and is generally easy to see as distressed.
- They may also present as blank or disengaged. They may isolate themselves, be unable to make eye contact with you, be reluctant to join in with things they used to enjoy or have a flat facial expression or monotone voice. This is known as hypoarousal and is much easier to miss than hyperarousal.
- People with learning disabilities may tend to present in one of, or both of these ways when they are distressed. They may find it difficult to communicate about a specific problem, or how they are feeling emotionally. This means it is really important for us to be aware of the ways they generally show distress, including the signs of hypoarousal, so that we can respond.
- People experiencing hyper or hypo arousal may need support to reduce their distress and bring them back to their Window of Tolerance – this means a space where they are clear-headed and can think and feel at the same time. It is important to refer to care plans and established strategies which are known to help the person you are supporting, but here are some principles and ideas it might be useful to consider:
Being with someone and sharing their pain
When there is no simple solution to distress, there is a real value in remaining physically present with the distressed person – and in doing so, supporting them to remain with the distress. Validating their feelings (for example, saying things like “this is really sad, I can understand that you feel really sad”) can help people to feel seen and that it is safe for them to express emotions. This video explains it well – https://www.youtube.com/watch?v=l2zLCCRT-nE
Grounding
This involves helping the person to be present in the current moment rather than worrying about the future. There are many grounding activities, and these can be very simple and are often connected to the five senses, such as asking the person to look for the things in a room that are green or drawing attention to what it feels like to have their feet on the ground. This helps the person remember that they are safe right now.
Time
It is important to remember that over time, the way we feel about things changes as our brain is able to process and make sense of things. There is no magic fix to the distress some might feel in this situation, but over time it may affect them less. For someone with a learning disability, they might need more time or repeated explanations. It is important to allow processing time and space for questions. Having conversations early can help start this process sooner, and covering important topics at the person’s own pace – such as what happens when we die, what hospices do, medication in an accessible way etc can help PWLD feel more aware and less anxious about what might happen.
Acceptance
Sometimes, a person will accept their diagnosis and be able to make plans for how they spend their time and make choices about what a good death looks like for them. However, some people won’t be able to do this. This may be because it is too big to think about, or the emotion is too much to process. By showing compassion, we support the person in moving through emotions at their own pace.
Looking after yourself
Working with people at this time of their lives can be emotional for staff caring for them. It is important to allow some space when things start to feel heavy, both for yourselves and your colleagues.
Understanding the death of someone else
It can be very distressing for people with learning disabilities when death is not mentioned. For example, if another person in your care setting dies, it can feel very confusing if they disappear and this is not spoken about. It is good to have an open conversation to enable expression of their feelings in a safe way.
If the person you are working with is in severe distress which does not resolve and it is having a significant impact on their life, please contact their GP and make a referral to the Community Learning Disability Nursing service. (See contact details in Appendix 4)